Zollinger Atlas Of Surgical Operations Free Download
| Tracheotomy | |
|---|---|
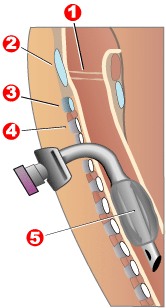 Completed tracheotomy: 1 – Song folds 5 – Balloon cuff | |
| ICD-10-PCS | 0B110F4 |
| ICD-nine-CM | 31.1 |
| MeSH | D014140 |
| MedlinePlus | 002955 |
Tracheotomy (, UK also ), or tracheostomy, is a surgical process which consists of making an incision (cut) on the anterior aspect (front) of the cervix and opening a direct airway through an incision in the trachea (windpipe). The resulting stoma (pigsty) can serve independently as an airway or as a site for a tracheal tube or tracheostomy tube [i] to be inserted; this tube allows a person to breathe without the utilize of the nose or mouth.
Etymology and terminology [edit]

Effigy A shows a side view of the cervix and the right placement of a tracheostomy tube in the trachea, or windpipe. Figure B shows an external view of a patient who has a tracheostomy.
The etymology of the word tracheotomy comes from two Greek words: the root tom- (from Greek τομή tomḗ) meaning "to cut", and the word trachea (from Greek τραχεία tracheía).[two] The word tracheostomy, including the root stom- (from Greek στόμα stóma) pregnant "mouth," refers to the making of a semi-permanent or permanent opening, and to the opening itself. Some sources offer different definitions of the above terms. Function of the ambiguity is due to the uncertainty of the intended permanence of the stoma (hole) at the time information technology is created.[3]
Indications [edit]
At that place are four main reasons why someone would receive a tracheotomy:[three]
- Emergency airway admission
- Airway access for prolonged mechanical ventilation
- Functional or mechanical upper airway obstacle
- Decreased/incompetent clearance of tracheobronchial secretions
Bypassing upper airway blockages [edit]
In the astute (brusque term) setting, indications for tracheotomy include such conditions equally severe facial trauma, tumors of the head and cervix (e.g., cancers, branchial crack cysts), and acute angioedema and inflammation of the caput and neck. In the context of failed tracheal intubation, either tracheotomy or cricothyrotomy may be performed.[ citation needed ]
Long term ventilation [edit]

In the chronic (long term) setting, indications for tracheotomy include the demand for long-term mechanical ventilation and tracheal toilet (e.g. comatose patients, or extensive surgery involving the head and neck). Tracheotomy may issue in a meaning reduction in the administration of sedatives and vasopressors, as well as the duration of stay in the intensive care unit (ICU).[four]
In extreme cases, the process may be indicated as a treatment for severe obstructive slumber apnea (OSA) seen in patients intolerant of continuous positive airway pressure (CPAP) therapy. The reason tracheostomy works well for OSA is considering information technology is the only surgical procedure that completely bypasses the upper airway. This process was commonly performed for obstructive sleep apnea until the 1980s, when other procedures such as the uvulopalatopharyngoplasty, genioglossus advancement, and maxillomandibular advancement surgeries were described equally alternative surgical modalities for OSA.
Timing (early vs tardily) [edit]
If prolonged ventilation is required, tracheostomy is usually considered. The timing of this process is dependent on the clinical situation and an private'due south preference. An international multicenter study in 2000 adamant that the median time between starting mechanical ventilation and receiving a tracheostomy was 11 days.[5] Although the definition varies depending on hospital and provider, early on tracheostomy can be considered to be less than x days (2 to 14 days) and late tracheostomy to be x days or more.
A meta-analysis in 2015 revealed improved outcomes from early tracheostomy compared to late tracheostomy, including decreased number of days in the intensive care unit (ICU), decreased utilize of allaying medications, and decreased mortality rates.[half dozen] However, another meta-assay done the same twelvemonth did not find whatever significant differences betwixt early on and belatedly tracheostomy other than decreased amount of fourth dimension on sedative medications.[vii] Given the minimal or unproven benefit of early tracheostomy, many wellness care providers opt to wait at least 10 days to prevent unnecessary surgeries or prolonged mechanical ventilation if extubation, removal of the breathing tube, is an option.
Parts [edit]

An outer cannula (top item) with inflatable gage (top right), an inner cannula (heart item) and an obturator (bottom item)
A tracheostomy tube may be single or dual lumen, and also cuffed or uncuffed. A dual lumen tracheostomy tube consists of an outer cannula or main shaft, an inner cannula, and an obturator. The obturator is used when inserting the tracheostomy tube to guide the placement of the outer cannula and is removed once the outer cannula is in identify. The outer cannula remains in place but, because of the buildup of secretions, there is an inner cannula that may be removed for cleaning after use or information technology may be replaced. Single lumen tracheostomy tubes do not have a removable inner cannula, suitable for narrower airways. Cuffed tracheostomy tubes have inflatable balloons at the end of the tube to secure them in place. A tracheostomy tube may be fenestrated with one or several holes to let air through the larynx, allowing speech.[8]
Passy-Muir valve [edit]
Special tracheostomy tube valves (such as the Passy-Muir valve[9]) have been created to assistance people in their speech communication. The patient can inhale through the unidirectional tube. Upon expiration, pressure causes the valve to close, redirecting air around the tube, past the vocal folds, producing audio.[10]
Surgical procedure [edit]
Instruments [edit]
By the late 19th century, some surgeons had become proficient in performing the tracheotomy process. The main instruments used were:
"Two small scalpels, ane short grooved managing director, a tenaculum, 2 aneurysm needles which may exist used every bit retractors, one pair of artery forceps, haemostatic forceps, ii pairs of dissecting forceps, a pair of scissors, a precipitous-pointed tenotome, a pair of tracheal forceps, a tracheal dilator, tracheotomy tubes, ligatures, sponges, a flexible catheter, and feathers".[11]
Haemostatic forceps were used to control bleeding from separated vessels that were not ligatured because of the urgency of the operation. Generally, they were used to expose the trachea by clamping the isthmus thyroid gland on both sides. To open the trachea physically, a precipitous-pointed tentome allowed the surgeon hands to place the ends into the opening of the trachea. The thin points permitted the md a amend view of his incision. Tracheal dilators, such as the "Golding Bird", were placed through the opening and so expanded by "turning the screw to which they are attached". Tracheal forceps, as displayed on the correct, were commonly used to extract foreign bodies from the larynx. The optimum tracheal tube at the time caused very picayune damage to the trachea and "mucus membrane" [sic].[11]
The best position for a tracheotomy was and still is one that forces the neck into the biggest prominence. Ordinarily, the patient is laid on their back on a table with a absorber placed under their shoulders to prop them upward. The artillery are restrained to ensure they would not get in the manner afterward.[11] The tools and techniques used today in tracheotomies have come a long way. The tracheotomy tube placed into the incision through the windpipe comes in various sizes, thus allowing a more comfortable fit and the ability to remove the tube in and out of the throat without disrupting support from a animate motorcar. In today's earth general anesthesia is used when performing these surgeries, which makes it much more tolerable for the patient.
Significant improvements to surgical instruments for tracheotomy include the direct suction tracheotomy tube invented by Josephine G. Fountain (RN); she was awarded patent no. 3039469 in 1962 for the direct suction tracheotomy tube, which improved the ways mucus could be cleared from the trachea and increased patient breathing and comfort.[12]
Open surgical tracheotomy (OST) [edit]
The typical procedure done is the open surgical tracheotomy (OST) and is unremarkably washed in a sterile operating room. The optimal patient position involves a cushion under the shoulders to extend the cervix. Commonly a transverse (horizontal) incision is fabricated two fingerbreadths higher up the suprasternal notch. Alternatively, a vertical incision can be made in the midline of the neck from the thyroid cartilage to but above the suprasternal notch. Skin, subcutaneous tissue, and strap muscles (a specific group of cervix muscles) are retracted bated to betrayal the thyroid isthmus, which can exist cut or retracted upwards. After proper identification of the cricoid cartilage and placement of a tracheal hook to steady the trachea and pull it forrad, the trachea is cut open up, either through the space betwixt cartilage rings or vertically across multiple rings (cruciate incision). Occasionally a section of a tracheal cartilage ring may be removed to brand insertion of the tube easier. One time the incision is made, a properly sized tube is inserted. The tube is connected to a ventilator and adequate ventilation and oxygenation is confirmed. The tracheotomy apparatus is then attached to the neck with tracheotomy ties, pare sutures, or both.[xiii] [14]
Percutaneous dilatational tracheotomy (PDT) [edit]
The Griggs and Ciaglia Blue Rhino techniques are the ii main techniques in current use. A number of comparison studies have been undertaken between these ii techniques with no articulate differences emerging[15] An advantage of PDT over OST is the ability to perform the procedure at the patient's bedside. This significantly decreases costs and time/people-ability needed for an operating room (OR) procedure.[14]
Ciaglia technique [edit]
While there were some before false starts, the first widely accepted percutaneous tracheotomy technique was described by Pat Ciaglia, a New York surgeon, in 1985. This technique involves a serial of sequential dilatations using a set of seven dilators of progressively larger size.[16]
Griggs technique [edit]
The next widely used technique was adult in 1989 by Beak Griggs, an Australian intensive care specialist. This technique involves the employ of a specially modified pair of forceps with a central hole enabling them to laissez passer over a guidewire enabling the performance of the main dilation in a single step.[17]
Fantoni technique [edit]
In 1995, Fantoni developed a translaryngeal arroyo of percutaneous tracheostomy which involves passing a guidewire through the larynx and over it railroading a tracheostomy tube with a cone shaped construction. It is also known equally the In-and-out process.[18] This technique is characterized by the exclusive procedure to behave out the stoma. A cone of soft plastic textile, welded to a flexible cannula, is passed into the trachea through the glottis, and so extracted outside of the neck through the pretracheal layers. The direction of this dilational maneuver is from the inside of the tracheal lumen to the outside of the neck (In/Out) and therefore completely opposite to the Out/In of other traditional percutaneous tracheostomies. The cone is then separated from the cannula, which results in it being positioned in the trachea. [18]
This method ensures considerable advantages, 2 of which are of particular importance: the removal of the risk of perforation of the posterior wall and the reduction of local trauma to a level that is unlikely to be farther lowered. The use of a ventilation catheter during the fourth dimension of the procedure allows total control of the airway and to extend the indications of the technique to patients with severe respiratory failure.
Ciaglia blue rhinoceros technique [edit]
A variant of the original Ciaglia technique, using a single tapered dilator known every bit a "blue rhino", is the most commonly used of these newer techniques and has largely taken over from the early multiple dilator technique.
Ambesh SP (2005) introduced a T-Trach kit (T-Dagger) which contains a T-shaped dilator with an elliptical shaft. The shaft of the dilator is marked in its length according to the sizes of tracheostomy tube to be introduced and has a number of holes. This T-shaped dilator provides better grip during its introduction and its elliptical shaft forms a calibrated tracheal stoma between two tracheal rings and minimizes tracheal band fracture.[xix]
Contraindications [edit]
In that location are a few absolute contraindications for percutaneous tracheostomy:[ii]
- Active infection at the site of tracheostomy
- Uncontrolled bleeding disorder
- Unstable cardiopulmonary status (stupor, extremely poor ventilatory status)
- Patient unable to stay still
- Aberrant anatomy of the tracheolaryngeal structures
Percutaneous tracheostomy is typically avoided in pediatric patients. Percutaneous tracheostomy can exist safely performed in the presence of:[20]
- Obesity
- Neutropenia
- History of sternotomy
- Spinal string injury
- Repeat tracheostomy
Risks and complications [edit]
As with almost other surgical procedures, some cases are more difficult than others. Surgery on children is more than hard because of their smaller size. Difficulties such equally a brusk cervix and bigger thyroid glands make the trachea hard to open.[11] There are other difficulties with patients with irregular necks, the obese, and those with a large goitre.
Potential complications [edit]
The many possible complications include hemorrhage, loss of airway, subcutaneous emphysema, wound infections, stomal cellulites, fracture of tracheal rings, poor placement of the tracheostomy tube, and bronchospasm.[twenty]
Early on complications include infection, hemorrhage, pneumomediastinum, pneumothorax, tracheoesophageal fistula, recurrent laryngeal nerve injury, and tube displacement. Delayed complications include tracheal-innominate avenue fistula, tracheal stenosis, delayed tracheoesophageal fistula, and tracheocutaneous fistula.[thirteen]
A 2013 systematic review (published cases from 1985 to April 2013) studied the complications and risk factors of percutaneous dilatational tracheostomy (PDT), identifying major causes of fatality to exist hemorrhage (38.0%), airway complications (29.6%), tracheal perforation (xv.5%), and pneumothorax (5.6%)[21] A similar systematic review in 2017 (cases from 1990 to 2015) studying fatality in both open surgical tracheotomy (OST) and PDT identified like rates of mortality and causes of death between the two techniques.[22]
Hemorrhage [edit]
Hemorrhage is rare, only the most likely cause of fatality after a tracheostomy. Information technology unremarkably occurs due to a tracheoarterial fistula, an abnormal connection betwixt the trachea and nearby blood vessels, and most commonly manifests between 3 days to 6 weeks later on the procedure is done. Fistulas can upshot from incorrectly positioned equipment, high gage pressures causing force per unit area sores or mucosal damage, a low surgical trachea site, repetitive neck movement, radiotherapy, or prolonged intubation.[23]
A potential take chances factor identified in a 2013 systematic review of the percutaneous technique was the lack of bronchoscopic guidance. Use of the bronchoscope, an instrument inserted through a patient's mouth for internal visualization of the airway, can help with proper placement of instruments and better visualization of anatomical structures. However, this tin can besides be dependent on the skills and familiarity of the surgeon with both the procedure and the patient'due south anatomy.[21]
Airway complications [edit]
There are a multitude of potential complications related to the airway. The main causes of mortality during PDT include dislodgment of the tube, loss of airway during process and misplacement of the tube.[21] Ane of the more urgent complications include displacement or dislodgment of the tracheotomy tube, either spontaneously or during a tube change. Although uncommon (< 1/1000 tracheostomy tube days), the associated fatality is high due to the loss of airway.[24] Due to the seriousness of such a situation, individuals with a tracheotomy tube should consult with their healthcare providers to have a specific, written, emergency intubation and tracheostomy recannulation (reinsertion) program prepared in accelerate.
Long-term tracheal stenosis [edit]
Tracheal stenosis, otherwise known equally an abnormal narrowing of the airway, is a possible long term complication. The about common symptom of stenosis is gradually-worsening difficulty with animate (dyspnea). Still incidence is low, ranging from 0.vi to two.8% with increased rates if major bleeding or wound infections are nowadays. A 2016 systematic review identified a higher rate of tracheal stenosis in individuals who underwent a surgical tracheostomy, as compared to PDT, however the difference was non statistically significant.[25]
Complication rates [edit]
A 2000 Castilian study of bedside percutaneous tracheostomy reported overall complication rates of 10–15% and a procedural mortality of 0%,[26] which is comparable to those of other series reported in the literature from kingdom of the netherlands[27] [28] and the United States.[29] [thirty] A 2013 systematic review calculated procedural mortality to be 0.17% or 1 in 600 cases.[21] Multiple systematic reviews identified no significant difference in rates of mortality, major bleeding, or wound infection between the percutaneous or open surgical methods.[25] [22]
Specifically a 2017 systematic review calculated the near common causes of decease and their frequencies, out of all tracheotomies, to be hemorrhage (OST: 0.26%, PDT: 0.19%), loss of airway (OST: 0.21%, PDT: 0.20%), and misplacement of tube (OST: 0.eleven%, PDT: 0.20%).[22]
A 2003 American cadaveric study identified multiple tracheal band fractures with the Ciaglia Blue Rhino technique as a complication occurring in 100% of their small series of cases.[31] The comparative report above as well identified ring fractures in ix of 30 alive patients[15] while another small series identified band fractures in five of their 20 patients.[32] The long term significance of tracheal ring fractures is unknown.[ citation needed ]
Alternatives [edit]
Biphasic cuirass ventilation is a class of not-invasive mechanical ventilation that tin can in many cases permit patients an alternative manner of respiratory support, assuasive patients to avoid an invasive tracheostomy and its many complications. While this method has not been proven to aid in every case, information technology has been shown to be an effective alternative for many.[33]
Routine care [edit]
Suctioning [edit]
Caring for a tracheotomy mostly includes suctioning to foreclose occlusions and replacing supplies, such every bit replacement of the inner cannula and/or suction devices. Because of the lack of filtering and humidifying by the nose and the ineffective cough mechanism, at that place is a buildup of secretions. Suctioning is only performed when clinically necessary because there are many potential risks. Risks include hypoxia and and then suctioning is limited to x to 20 seconds at a time and the patient is hyperoxygenated just before and after suctioning. Risks also include atelectasis, or collapsing lung tissue from high suction pressure, and so pressure is express to eighty–120 mm Hg. Risks besides include tissue impairment. The suction catheter is inserted no more than 1 cm past the length of the tube to avoid contact with trachea tissue. Suctioning is only washed during withdrawing the catheter at least i/two-inch. Risks also include infection.[8]
History [edit]

A tracheostomy from prior to the 20th century
Ancient Arab republic of egypt [edit]
Tracheotomy was first potentially depicted on Egyptian artifacts in 3600 BC.[34] Hippocrates condemned the practice of tracheotomy equally incurring an unacceptable run a risk of damage to the carotid artery. Alarm confronting the possibility of death from inadvertent laceration of the carotid artery during tracheotomy, he instead advocated the practice of tracheal intubation.[20]
Despite the concerns of Hippocrates, information technology is believed that an early tracheotomy was performed by Asclepiades of Bithynia, who lived in Rome around 100 BC.[35] Galen and Aretaeus, both of whom lived in Rome in the second century AD, credit Asclepiades as being the first physician to perform a non-emergency tracheotomy. Antyllus, another Roman-era Greek physician of the 2nd century AD, supported tracheotomy when treating oral diseases. He refined the technique to be more similar to that used in modern times, recommending that a transverse incision exist fabricated between the third and fourth tracheal rings for the treatment of life-threatening airway obstruction.[20]
Medieval Islamic globe [edit]
In 1000, Abu al-Qasim al-Zahrawi (936–1013), an Arab who lived in Standard arabic Spain, published the 30-volume Kitab al-Tasrif, the outset illustrated piece of work on surgery. He never performed a tracheotomy, just he did care for a slave girl who had cut her ain throat in a suicide try. Al-Zahrawi (known to Europeans as Albucasis) sewed up the wound and the girl recovered, thereby proving that an incision in the larynx could heal. Circa Advert 1020, Avicenna (980–1037) described tracheal intubation in The Canon of Medicine in gild to facilitate animate.[36] The get-go correct description of the tracheotomy operation for treatment of asphyxiation was described by Ibn Zuhr (1091–1161) in the 12th century. According to Mostafa Shehata, Ibn Zuhr (also known every bit Avenzoar) successfully practiced the tracheotomy procedure on a goat, justifying Galen's approval of the functioning.[37]
16th–18th centuries [edit]
The European Renaissance brought with it meaning advances in all scientific fields, particularly surgery. Increased knowledge of anatomy was a major gene in these developments. Surgeons became increasingly open to experimental surgery on the trachea. During this period, many surgeons attempted to perform tracheotomies, for various reasons and with various methods. Many suggestions were put forward, but little actual progress was fabricated toward making the process more successful. The tracheotomy remained a unsafe operation with a very low success rate,[ quantify ] and many surgeons even so considered the tracheotomy to exist a useless and dangerous procedure. The high mortality rate[ quantify ] for this operation, which had not improved, supported their position.
From the menstruum 1500 to 1832 in that location are only 28 known reports of tracheotomy.[38] In 1543, Andreas Vesalius (1514–1564) wrote that tracheal intubation and subsequent artificial respiration could be life-saving. Antonio Musa Brassavola (1490–1554) of Ferrara treated a patient suffering from peritonsillar abscess past tracheotomy after the patient had been refused past barber surgeons. The patient manifestly made a consummate recovery, and Brassavola published his account in 1546. This functioning has been identified as the first recorded successful tracheostomy, despite many aboriginal references to the trachea and perhaps to its opening.[38] Ambroise Paré (1510–1590) described suture of tracheal lacerations in the mid-16th century. One patient survived despite a concomitant injury to the internal jugular vein. Another sustained wounds to the trachea and esophagus and died.

Towards the end of the 16th century, anatomist and surgeon Hieronymus Fabricius (1533–1619) described a useful technique for tracheotomy in his writings, although he had never actually performed the performance himself. He brash using a vertical incision and was the first to introduce the idea of a tracheostomy tube. This was a straight, brusque cannula that incorporated wings to forbid the tube from advancing too far into the trachea. He recommended the operation only equally a final resort, to exist used in cases of airway obstruction by foreign bodies or secretions. Fabricius' clarification of the tracheotomy procedure is like to that used today. Julius Casserius (1561–1616) succeeded Fabricius as professor of anatomy at the Academy of Padua and published his own writings regarding technique and equipment for tracheotomy. Casserius recommended using a curved silver tube with several holes in it. Marco Aurelio Severino (1580–1656), a skilful surgeon and anatomist, performed multiple successful tracheotomies during a diphtheria epidemic in Naples in 1610, using the vertical incision technique recommended by Fabricius. He likewise developed his ain version of a trocar.[39]
In 1620 the French surgeon Nicholas Habicot (1550–1624), surgeon of the Duke of Nemours and anatomist, published a report of four successful "bronchotomies" which he had performed.[40] One of these is the first recorded instance of a tracheotomy for the removal of a foreign body, in this instance a blood jell in the larynx of a stabbing victim. He too described the commencement tracheotomy to exist performed on a pediatric patient. A 14-year-old boy swallowed a handbag containing ix gold coins in an attempt to forbid its theft by a highwayman. The object became lodged in his esophagus, obstructing his trachea. Habicot suggested that the operation might also be effective for patients suffering from inflammation of the larynx. He developed equipment for this surgical process which displayed similarities to mod designs (except for his use of a single-tube cannula).[ citation needed ]
Sanctorius (1561–1636) is believed to be the first to use a trocar in the operation, and he recommended leaving the cannula in place for a few days following the operation.[41] Early tracheostomy devices are illustrated in Habicot's Question Chirurgicale [twoscore] and Julius Casserius' posthumous Tabulae anatomicae in 1627.[42] Thomas Fienus (1567–1631), Professor of Medicine at the Academy of Louvain, was the first to employ the discussion "tracheotomy" in 1649, but this term was not commonly used until a century later on.[43] Georg Detharding (1671–1747), professor of anatomy at the University of Rostock, treated a drowning victim with tracheostomy in 1714.[44] [45] [46]
19th century [edit]
In the 1820s, the tracheotomy began to be recognized as a legitimate ways of treating severe airway obstruction. In 1832, French physician Pierre Bretonneau employed information technology as a last resort to treat a instance of diphtheria.[47] In 1852, Bretonneau'south student Armand Trousseau reported a serial of 169 tracheotomies (158 of which were for croup, and eleven for "chronic maladies of the larynx")[48] In 1858, John Snow was the beginning to report tracheotomy and cannulation of the trachea for the administration of chloroform anesthesia in an animal model.[49] In 1871, the German surgeon Friedrich Trendelenburg (1844–1924) published a newspaper describing the first successful constituent human tracheotomy to be performed for the purpose of administration of general anesthesia.[fifty] In 1880, the Scottish surgeon William Macewen (1848–1924) reported on his utilize of orotracheal intubation as an alternative to tracheotomy to allow a patient with glottic edema to breathe, equally well equally in the setting of general anesthesia with chloroform.[51] [52] At concluding, in 1880 Morell Mackenzie's volume discussed the symptoms indicating a tracheotomy and when the operation is absolutely necessary.[20]
20th century [edit]

Laryngeal structures, trachea (1 - 4) and invasive procedures (A - B) (one) Thyroid cartilage (2) Cricothyroid ligament (3) Cricoid cartilage (4) Trachea (A) Cricothyrotomy (B) Tracheotomy
In the early 20th century, physicians began to utilise the tracheotomy in the treatment of patients afflicted with paralytic poliomyelitis who required mechanical ventilation. However, surgeons continued to debate various aspects of the tracheotomy well into the 20th century. Many techniques were described and employed, along with many different surgical instruments and tracheal tubes. Surgeons could not seem to reach a consensus on where or how the tracheal incision should be made, arguing whether the "loftier tracheotomy" or the "low tracheotomy" was more than benign. The currently used surgical tracheotomy technique was described in 1909 by Chevalier Jackson of Pittsburgh, Pennsylvania. Jackson emphasised the importance of postoperative intendance, which dramatically reduced the expiry charge per unit. By 1965, the surgical anatomy was thoroughly and widely understood, antibiotics were widely available and useful for treating postoperative infections, and other major complications had besides become more manageable.
Lodge and culture [edit]
Notable individuals who have or accept had a tracheotomy include Stephen Hawking, Christopher Reeve,[53] Roy Horn, William Rehnquist, Gabby Giffords, and many others.[54]
In popular media [edit]
Beyond movies and TV shows, there are many situations where an emergency procedure is done on an individual'south neck to re-establish an airway. An instance is in the 2008 horror, Saw V, in which a grapheme being drowned from the cervix upwardly performs a manual tracheotomy, stabbing his cervix with a pen to create an airway to exhale through. The nigh common procedure is a cricothyrotomy (or "crike"), which is an incision through the skin and cricothyroid membrane. This is often confused or misnamed every bit a tracheotomy (or "trach") and vice versa. However, they are quite dissimilar based on location of the opening and length of time the alternate airway is needed.
See likewise [edit]
- Cricothyrotomy
- Laryngotomy
- Listing of surgeries by type
References [edit]
- ^ Molnar, Heather. "Types of Tracheostomy Tubes".
- ^ a b Romaine F. Johnson (6 March 2003). "Adult Tracheostomy". Houston, Texas: Department of Otolaryngology–Head and Cervix Surgery, Baylor College of Medicine. Archived from the original on 17 May 2008.
- ^ a b Jonathan P Lindman; Charles Due east Morgan (vii June 2010). "Tracheostomy". WebMD.
- ^ Eberhardt, Lars Karl (2008). Dilatational Tracheostomy on an Intensive Care Unit (Dissertation). Universität Ulm.
- ^ Esteban A, Anzueto A, Alía I, Gordo F, Apezteguía C, Pálizas F, Cide D, Goldwaser R, Soto Fifty, Bugedo G, Rodrigo C, Pimentel J, Raimondi G, Tobin MJ (May 2000). "How is mechanical ventilation employed in the intensive intendance unit? An international utilization review". American Journal of Respiratory and Critical Care Medicine. 161 (v): 1450–8. doi:10.1164/ajrccm.161.v.9902018. PMID 10806138.
- ^ Hosokawa Grand, Nishimura Thousand, Egi M, Vincent JL (December 2015). "Timing of tracheotomy in ICU patients: a systematic review of randomized controlled trials". Disquisitional Care. nineteen: 424. doi:ten.1186/s13054-015-1138-8. PMC4669624. PMID 26635016.
- ^ Szakmany T, Russell P, Wilkes AR, Hall JE (March 2015). "Event of early on tracheostomy on resource utilization and clinical outcomes in critically ill patients: meta-assay of randomized controlled trials". British Journal of Anaesthesia. 114 (3): 396–405. doi:ten.1093/bja/aeu440. PMID 25534400.
- ^ a b Taylor, C. R., Lillis, C., LeMone, P., Lynn, P. (2011) Fundamentals of nursing: The fine art and scientific discipline of nursing care. Philadelphia: Lippincott Williams & Wilkins, page 1382–1383, 1404.
- ^ Passy Five, Baydur A, Prentice Due west, Darnell-Neal R (June 1993). "Passy-Muir tracheostomy speaking valve on ventilator-dependent patients". The Laryngoscope. 103 (6): 653–viii. doi:ten.1288/00005537-199306000-00013. PMID 8502098. S2CID 22397705.
- ^ Cullen JH (June 1963). "An evaluation of tracheostomy in pulmddddddonary emphysema". Annals of Internal Medicine. 58 (6): 953–threescore. doi:x.7326/0003-4819-58-6-953. PMID 14024192.
- ^ a b c d Rosen H (January 1897). "On enactment". Journal of the American Psychoanalytic Association. forty (4): 1228–9. doi:ten.1097/00000441-189701000-00008. PMC1430766. PMID 1430766.
- ^ US patent 3039469
- ^ a b Lalwani, Anil K. (2012). CURRENT Diagnosis & Treatment in Otolaryngology—Head & Neck Surgery, 3e. New York, NY: McGraw-Hill. pp. Yu KY. Chapter 38. Airway Management & Tracheotomy. ISBN978-0-07-162439-viii.
- ^ a b Ellison, Eastward. Christopher; Zollinger, Jr, Robert G. (2016). Zollinger's Atlas of Surgical Operations, 10th edition. New York, NY: McGraw-Hill. pp. Chapter 120- Tracheotomy, Chapter 121- Tracheotomy, Percutaneous Dilational. ISBN978-0-07-179755-nine.
- ^ a b Ambesh SP, Pandey CK, Srivastava S, Agarwal A, Singh DK (December 2002). "Percutaneous tracheostomy with single dilatation technique: a prospective, randomized comparing of Ciaglia blue rhino versus Griggs' guidewire dilating forceps". Anesthesia and Analgesia. 95 (6): 1739–45, table of contents. doi:10.1097/00000539-200212000-00050. PMID 12456450. S2CID 22222451.
- ^ Ciaglia P, Firsching R, Syniec C (June 1985). "Constituent percutaneous dilatational tracheostomy. A new simple bedside process; preliminary study". Chest. 87 (half-dozen): 715–9. doi:ten.1378/breast.87.half dozen.715. PMID 3996056. S2CID 27125996.
- ^ Griggs WM, Worthley LI, Gilligan JE, Thomas PD, Myburg JA (June 1990). "A simple percutaneous tracheostomy technique". Surgery, Gynecology & Obstetrics. 170 (6): 543–5. PMID 2343371.
- ^ a b "Translaryngeal Tracheostomy- TLT Fantoni method". www.translaryngealtracheostomyfantoni.it. Archived from the original on 11 September 2017. Retrieved 21 December 2018.
- ^ Ambesh SP, Tripathi Grand, Pandey CK, Pant KC, Singh PK (July 2005). "Clinical evaluation of the "T-Dagger": a new bedside percutaneous dilational tracheostomy device". Amazement. sixty (7): 708–xi. doi:10.1111/j.1365-2044.2005.04236.x. PMID 15960723. S2CID 42851409.
- ^ a b c d e Ferlito A, Rinaldo A, Shaha AR, Bradley PJ (Dec 2003). "Percutaneous tracheotomy". Acta Oto-Laryngologica. 123 (9): 1008–12. doi:x.1080/00016480310000485. PMID 14710900. S2CID 23470798.
- ^ a b c d Simon M, Metschke M, Braune SA, Püschel Thousand, Kluge S (October 2013). "Death afterward percutaneous dilatational tracheostomy: a systematic review and analysis of take chances factors". Disquisitional Intendance. 17 (5): R258. doi:10.1186/cc13085. PMC4056379. PMID 24168826.
- ^ a b c Klemm E, Nowak AK (April 2017). "Tracheotomy-Related Deaths". Deutsches Ärzteblatt International. 114 (16): 273–279. doi:10.3238/arztebl.2017.0273. PMC5437259. PMID 28502311.
- ^ Grant CA, Dempsey G, Harrison J, Jones T (January 2006). "Tracheo-innominate avenue fistula subsequently percutaneous tracheostomy: three example reports and a clinical review". British Journal of Amazement. 96 (ane): 127–31. doi:10.1093/bja/aei282. PMID 16299043.
- ^ Rajendram (2017). "Tracheostomy tube deportation: An update on emergency airway management". Indian Periodical of Respiratory Intendance. six (2): 800. doi:10.4103/ijrc.ijrc_12_17.
- ^ a b Dempsey, Ged A.; Morton, Ben; Hammell, Clare; Williams, Lisa T.; Smith, Catrin Tudur; Jones, Terence (1 March 2016). "Long-term Consequence Following Tracheostomy in Disquisitional Intendance: A Systematic Review*". Critical Care Medicine. 44 (three): 617–628. doi:ten.1097/CCM.0000000000001382. ISSN 0090-3493. PMID 26584197. S2CID 32649464.
- ^ Añón JM, Gómez V, Escuela MP, De Paz 5, Solana LF, De La Casa RM, Pérez JC, Zeballos E, Navarro L (2000). "Percutaneous tracheostomy: comparison of Ciaglia and Griggs techniques". Critical Care. iv (2): 124–8. doi:10.1186/cc667. PMC29040. PMID 11056749.
- ^ van Heurn LW, van Geffen GJ, Brink PR (July 1996). "Clinical feel with percutaneous dilatational tracheostomy: report of 150 cases". The European Journal of Surgery = Acta Chirurgica. 162 (7): 531–v. PMID 8874159.
- ^ Polderman KH, Spijkstra JJ, de Bree R, Christiaans HM, Gelissen HP, Wester JP, Girbes AR (May 2003). "Percutaneous dilatational tracheostomy in the ICU: optimal arrangement, low complication rates, and clarification of a new complication". Chest. 123 (5): 1595–602. doi:10.1378/chest.123.5.1595. PMID 12740279.
- ^ Hill BB, Zweng TN, Maley RH, Charash We, Toursarkissian B, Kearney PA (August 1996). "Percutaneous dilational tracheostomy: report of 356 cases". The Periodical of Trauma. 41 (2): 238–43, word 243–4. doi:x.1097/00005373-199608000-00007. PMID 8760530.
- ^ Powell DM, Price PD, Forrest LA (February 1998). "Review of percutaneous tracheostomy". The Laryngoscope. 108 (2): 170–7. doi:10.1097/00005537-199802000-00004. PMID 9473064. S2CID 44972690.
- ^ Hotchkiss KS, McCaffrey JC (Jan 2003). "Laryngotracheal injury later percutaneous dilational tracheostomy in cadaver specimens". The Laryngoscope. 113 (one): sixteen–20. doi:x.1097/00005537-200301000-00003. PMID 12514375. S2CID 25597029.
- ^ Byhahn C, Lischke Five, Halbig Due south, Scheifler G, Westphal K (March 2000). "[Ciaglia bluish rhino: a modified technique for percutaneous dilatation tracheostomy. Technique and early on clinical results]" [Ciaglia blueish rhinoceros: a modified technique for percutaneous dilatation tracheostomy. Technique and early clinical results]. Der Anaesthesist (in German language). 49 (3): 202–6. doi:10.1007/s001010050815. PMID 10788989.
- ^ Linton DM (March 2005). "Cuirass ventilation: a review and update". Critical Care and Resuscitation. 7 (1): 22–eight. PMID 16548815.
- ^ Steven East. Sittig; James E. Pringnitz (February 2001). "Tracheostomy: evolution of an airway" (PDF). AARC Times: 48–51. Archived from the original (PDF) on 1 Apr 2017. Retrieved 5 June 2008.
- ^ Yapijakis, Christos (four July 2009). "Hippocrates of Kos, the father of clinical medicine, and Asclepiades of Bithynia, the begetter of molecular medicine. Review". In Vivo (Athens, Greece). 23 (4): 507–514. PMID 19567383 – via PubMed.
- ^ Patricia Skinner (2008). "Unani-tibbi". In Fundukian LJ (ed.). The Gale Encyclopedia of Alternative Medicine (third ed.). Farmington Hills, Michigan: Gale Cengage. ISBN978-1-4144-4872-5.
- ^ Mostafa Shehata (April 2003). "The Ear, Nose and Throat in Islamic Medicine" (PDF). Periodical of the International Society for the History of Islamic Medicine. 2 (iii): 2–five. ISSN 1303-667X.
- ^ a b Goodall, E.West. (1934). "The story of tracheostomy". British Journal of Children'south Diseases. 31: 167–76, 253–72.
- ^ Sedvall Grand, Farde L, Nybäck H, Pauli South, Persson A, Savic I, Wiesel FA (1960). "Recent advances in psychiatric brain imaging". Acta Radiologica. Supplementum. 374 (5179): 113–five. doi:x.1136/bmj.1.5179.1129. PMC1966956. PMID 1966956.
- ^ a b Nicholas Habicot (1620). Question chirurgicale par laquelle il est démonstré que le Chirurgien doit assurément practiquer 50'operation de la Bronchotomie, vulgairement dicte Laryngotomie, ou perforation de la fluste ou du polmon (in French). Paris: Corrozet. p. 108.
- ^ Sanctorii Sanctorii (1646). Sanctorii Sanctorii Commentaria in primum fen, primi libri canonis Avicennæ (in Latin). Venetiis: Apud Marcum Antonium Brogiollum. p. 1120. OL 15197097M.
- ^ Julius Casserius (Giulio Casserio) and Daniel Bucretius (1632). Tabulae anatomicae LXXIIX ... Daniel Bucretius ... Xx. que deerant supplevit & omnium explicationes addidit (in Latin). Francofurti: Impensis & coelo Matthaei Meriani. [ permanent expressionless link ]
- ^ Cawthorne T, Hewlett AB, Ranger D (June 1959). "Tracheostomy in a respiratory unit at a neurological hospital". Proceedings of the Royal Gild of Medicine. 52 (6): 403–v. doi:10.1177/003591575905200602. PMC1871130. PMID 13667911.
- ^ Georges Detharding (1745). "De methodo subveniendi submersis per laryngotomiam (1714)". In Von Ernst Ludwig Rathlef; Gabriel Wilhelm Goetten; Johann Christoph Strodtmann (eds.). Geschichte jetzlebender Gelehrten, als eine Fortsetzung des Jetzlebenden. Zelle: Berlegts Joachim Undreas Deek. p. 20.
- ^ Toll JL (January 1962). "The development of breathing machines". Medical History. half dozen (1): 67–72. doi:10.1017/s0025727300026867. PMC1034674. PMID 14488739.
- ^ Wischhusen HG, Schumacher GH (1977). "[Curriculum vitae of the professor of anatomy, botany and higher mathematics Georg Detharding (1671–1747) at the University of Rostock (writer's transl)]" [Curriculum vitae of the professor of anatomy, botany and higher mathematics Georg Detharding (1671–1747) at the University of Rostock]. Anatomischer Anzeiger (in German). 142 (i–2): 133–40. PMID 339777.
- ^ Armand Trousseau (1833). "Mémoire sur un cas de tracheotomie pratiquée dans la période extrème de croup". Journal des connaissances médico-chirurgicales. 1 (5): 41.
- ^ Armand Trousseau (1852). "Nouvelles recherches sur la trachéotomie pratiquée dans la période extrême du croup". In Jean Lequime and J. de Biefve (ed.). Annales de médecine belge et étrangère. Brussels: Imprimerie et Librairie Société Encyclographiques des Sciences Médicales. pp. 279–288.
- ^ Snowfall J (1858). "Fatal cases of inhalation of chloroform, Handling of suspended animation from chloroform". In Richardson BW (ed.). On chloroform and other anaesthetics: their action and administration. London: John Churchill. pp. 120–200, 251–62.
john snow.
- ^ Trendelenburg, F (1871). "Beiträge zu den Operationen an den Luftwegen" [Contributions to airways surgery]. Archiv für Klinische Chirurgie (in German). 12: 112–33.
- ^ Macewen W (July 1880). "General Observations on the Introduction of Tracheal Tubes by the Rima oris, Instead of Performing Tracheotomy or Laryngotomy". British Medical Journal. 2 (1021): 122–4. doi:10.1136/bmj.2.1021.122. PMC2241154. PMID 20749630.
- ^ Macewen W (July 1880). "Clinical Observations on the Introduction of Tracheal Tubes past the Mouth, Instead of Performing Tracheotomy or Laryngotomy". British Medical Periodical. 2 (1022): 163–5. doi:10.1136/bmj.2.1022.163. PMC2241109. PMID 20749636.
- ^ "Biography (Christopher Reeve Homepage)". www.chrisreevehomepage.com . Retrieved 19 December 2018.
- ^ "Famous people who take or have had Tracheostomies". www.tracheostomy.com . Retrieved 19 Dec 2018.
Farther reading [edit]
- Plotnikow GA, Roux N, Feld V, Gogniat E, Villalba D, Ribero NV, Sartore One thousand, Bosso M, Quiroga C, Leiva V, Scrigna M, Puchulu F, Distéfano E, Scapellato JL, Intile D, Planells F, Noval D, Buñirigo P, Jofré R, Nielsen ED (October 2013). "Evaluation of tracheal cuff pressure variation in spontaneously animate patients". International Journal of Critical Disease and Injury Science. 3 (four): 262–viii. doi:10.4103/2229-5151.124148. PMC3891193. PMID 24459624.
External links [edit]
- Tracheotomy Info (A community for tracheotomy-wearers and the people who love them) at tracheotomy.info
- Tracheostomy Products and Support (Online resource for tracheostomy products, supplies and support) at trachs.com
- Aaron's tracheostomy folio (Caring for a tracheostomy) at tracheostomy.com
- (Pictures with video clipping) at drtbalu.com
- Translaryngeal tracheostomy Archived 11 September 2017 at the Wayback Car
- "Tracheotomy" at Dorland's Medical Dictionary
- Smiths Medical Tracheostomy Training Videos
- A Video of Rescue Breathing for Laryngectomees and Neck Breathers
- "Book of Simplification Concerning Therapeutics and Diet", is a manuscript from 1497 that discusses tracheotomies
- An all inclusive resources about tracheostomy including articles and courses for medical professionals, caregivers and patients
- Site and weblog with information almost tracheostomies
- Global Tracheostomy Collaborative. International collaborative with resources for hospitals, caregivers, and patients about tracheostomies, including international research
- Dilatational Tracheostomy On An Intensive Care Unit
DOWNLOAD HERE
Posted by: steelefrond1975.blogspot.com


0 Comments